Chi-square help
Discussion


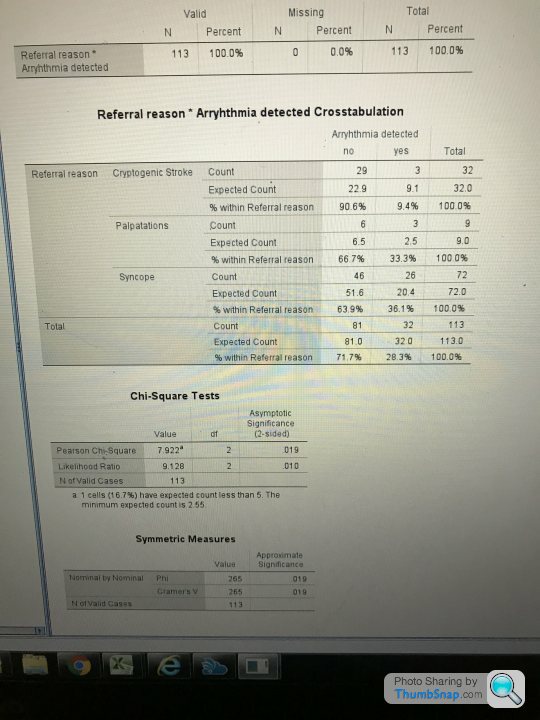
Am a bit unsure on the interpretation of a Chi-square test I’m trying to run. It’s related to a cardiac recorder fitted to different people, and seeing how referral reason might relate to detection of arrhythmia. Have used SPSS, and think have run the test okay:
So there P value comes out at 0.19, so that suggests there is an association between arrhythmia detection and referral reason. It’s more on the breakdown of where I’m more unsure. So for Cryptogenic stroke with no arrhythmia detected, the actual count was 29, as opposed to an expected of 22.9. Whereas for palpitations and syncope the actual count was less than the expected for no arrhythmia detected. So does that indicate that for stroke referrals significantly fewer arrhythmias are detected than for palpations and syncope? And as the detection count for syncope arrhythmias detected is higher than expected (26 compares to 20.4), then that referral group is seeing significantly more detected than other groups?
Another bit am wobbly on is homogeneity... So looking at the percentages the differences between stroke and palpitations are significantly different to one another? So are those between palpitations and syncope also significantly different, even though actual percentages pretty similar?
Apologies for waffle! Hope someone can try and point me down the right path on this one.
So there P value comes out at 0.19, so that suggests there is an association between arrhythmia detection and referral reason. It’s more on the breakdown of where I’m more unsure. So for Cryptogenic stroke with no arrhythmia detected, the actual count was 29, as opposed to an expected of 22.9. Whereas for palpitations and syncope the actual count was less than the expected for no arrhythmia detected. So does that indicate that for stroke referrals significantly fewer arrhythmias are detected than for palpations and syncope? And as the detection count for syncope arrhythmias detected is higher than expected (26 compares to 20.4), then that referral group is seeing significantly more detected than other groups?
Another bit am wobbly on is homogeneity... So looking at the percentages the differences between stroke and palpitations are significantly different to one another? So are those between palpitations and syncope also significantly different, even though actual percentages pretty similar?
Apologies for waffle! Hope someone can try and point me down the right path on this one.
All the chi squared test tells you is that there is a different pattern of referral reasons in people with arrhythmia detected, in comparison to those without.
Additional analysis is required to determine what is different about the referral patterns.
A common strategy for this type of post-hoc testing is to run a chi-squared test (or fisher exact test) between each pair of referral reasons and apply Bonferroni correction to the p values.
Additional analysis is required to determine what is different about the referral patterns.
A common strategy for this type of post-hoc testing is to run a chi-squared test (or fisher exact test) between each pair of referral reasons and apply Bonferroni correction to the p values.
Edited by WatchfulEye on Wednesday 1st April 18:18
Yes.
Your 3x2 chi-sq has highlighted that there is a difference between referrals and whether arrhythmia was present or not. You now have a reason to investigate further: is it because stroke gave way to syncope, or syncope gave way to palpitations, or did stroke give way to palpitations?
So, you now run these 3 separate 2x2 tests - taking care to correct the p-values. Note, that you have small numbers in some of the cells of the contingency table, so a chi-sq isn't a great test to use, especially in a 2x2 configuration - the Fisher test is a better option (although more conservative) - so run 3 Fisher tests on 2x2 tables, using Bonferroni correction to the p-value (i.e. if your Fisher test yields a p-value of 0.02, then you would multiply by 3, giving a corrected p-value of 0.06 which is not significant).
Your 3x2 chi-sq has highlighted that there is a difference between referrals and whether arrhythmia was present or not. You now have a reason to investigate further: is it because stroke gave way to syncope, or syncope gave way to palpitations, or did stroke give way to palpitations?
So, you now run these 3 separate 2x2 tests - taking care to correct the p-values. Note, that you have small numbers in some of the cells of the contingency table, so a chi-sq isn't a great test to use, especially in a 2x2 configuration - the Fisher test is a better option (although more conservative) - so run 3 Fisher tests on 2x2 tables, using Bonferroni correction to the p-value (i.e. if your Fisher test yields a p-value of 0.02, then you would multiply by 3, giving a corrected p-value of 0.06 which is not significant).
 Got it worked out I think! Much appreciated.
Got it worked out I think! Much appreciated. Gassing Station | Science! | Top of Page | What's New | My Stuff