Knee osteotomy
Discussion


Hi all, was just wondering if anyone has had a knee osteotomy? If so how long was recovery and did you make a return to sport/ active life?
I’ve had years of knee injuries from sport- resulting in no medial meniscus left after surgery last year. An X-ray shows I already have bad osteoarthritis so surgeon wants to limit me having a knee replacement as long as I can due to my age so has recommended osteotomy and another acl reconstruction. He had previously mentioned meniscus replacement along with the ACL but appears the osteoarthritis now stops this.
Thanks for any advice
I’ve had years of knee injuries from sport- resulting in no medial meniscus left after surgery last year. An X-ray shows I already have bad osteoarthritis so surgeon wants to limit me having a knee replacement as long as I can due to my age so has recommended osteotomy and another acl reconstruction. He had previously mentioned meniscus replacement along with the ACL but appears the osteoarthritis now stops this.
Thanks for any advice
I know of only one surgeon who offers this procedure (I suspect they are not the same person as your surgeon)
Given how rarely the procedure is performed, I can recall 2 patients who have required a below-knee amputation due to complications from the procedure.
A good friend of mine from medical school (who is an orthopaedic surgeon) expressed surprise that anyone still offers it as a treatment due to a lack of evidence of benefit
Clearly the above is personal anecdote, but even when I first saw one from the anaesthetic side, I couldn't understand why removing a chunk of bone was the answer to a catilage/meniscal problem.
There are plenty of other better-qualified people on here who could give better advice, but I'd be having a frank conversation with your surgeon again
REcent narrative I just found:https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8022014/
Given how rarely the procedure is performed, I can recall 2 patients who have required a below-knee amputation due to complications from the procedure.
A good friend of mine from medical school (who is an orthopaedic surgeon) expressed surprise that anyone still offers it as a treatment due to a lack of evidence of benefit
Clearly the above is personal anecdote, but even when I first saw one from the anaesthetic side, I couldn't understand why removing a chunk of bone was the answer to a catilage/meniscal problem.
There are plenty of other better-qualified people on here who could give better advice, but I'd be having a frank conversation with your surgeon again
REcent narrative I just found:https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8022014/
Edited by ucb on Wednesday 19th July 22:42
ucb said:
I know of only one surgeon who offers this procedure (I suspect they are not the same person as your surgeon)
Given how rarely the procedure is performed, I can recall 2 patients who have required a below-knee amputation due to complications from the procedure.
A good friend of mine from medical school (who is an orthopaedic surgeon) expressed surprise that anyone still offers it as a treatment due to a lack of evidence of benefit
Clearly the above is personal anecdote, but even when I first saw one from the anaesthetic side, I couldn't understand why removing a chunk of bone was the answer to a catilage/meniscal problem.
There are plenty of other better-qualified people on here who could give better advice, but I'd be having a frank conversation with your surgeon again
Slightly off topic but Is surgery still the wild West.Given how rarely the procedure is performed, I can recall 2 patients who have required a below-knee amputation due to complications from the procedure.
A good friend of mine from medical school (who is an orthopaedic surgeon) expressed surprise that anyone still offers it as a treatment due to a lack of evidence of benefit
Clearly the above is personal anecdote, but even when I first saw one from the anaesthetic side, I couldn't understand why removing a chunk of bone was the answer to a catilage/meniscal problem.
There are plenty of other better-qualified people on here who could give better advice, but I'd be having a frank conversation with your surgeon again
I had LARS ligaments to replace my PCL and MCL which failed in very short order.
The next surgeon said he'd never use them and they're banned in France, where they're made, no idea if that's true. He had a right old job removing them and said he ended up leaving some in.
Replaced with someone's achilles tendon which seems to be doing a slightly better job.
As a layman it's just impossible to tell who to believe.
ucb said:
I know of only one surgeon who offers this procedure (I suspect they are not the same person as your surgeon)
Given how rarely the procedure is performed, I can recall 2 patients who have required a below-knee amputation due to complications from the procedure.
A good friend of mine from medical school (who is an orthopaedic surgeon) expressed surprise that anyone still offers it as a treatment due to a lack of evidence of benefit
Clearly the above is personal anecdote, but even when I first saw one from the anaesthetic side, I couldn't understand why removing a chunk of bone was the answer to a catilage/meniscal problem.
There are plenty of other better-qualified people on here who could give better advice, but I'd be having a frank conversation with your surgeon again
REcent narrative I just found:https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8022014/
And whilst this has facts in it, and I don't doubt it as true. It is definitely NOT the picture.Given how rarely the procedure is performed, I can recall 2 patients who have required a below-knee amputation due to complications from the procedure.
A good friend of mine from medical school (who is an orthopaedic surgeon) expressed surprise that anyone still offers it as a treatment due to a lack of evidence of benefit
Clearly the above is personal anecdote, but even when I first saw one from the anaesthetic side, I couldn't understand why removing a chunk of bone was the answer to a catilage/meniscal problem.
There are plenty of other better-qualified people on here who could give better advice, but I'd be having a frank conversation with your surgeon again
REcent narrative I just found:https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8022014/
Edited by ucb on Wednesday 19th July 22:42
My unit is up to about 1500 of these operations and nobody lost a leg.
Where are you based, OP?
You just need to find the right experience.
Thanks for the replies. I’m in Scotland- believe I have a good surgeon who does quite a few of them. It just seem drastic for a meniscus problem but I’m getting a fair bit of stiffness/ pain already and guess a knee replacement wouldn’t be too many years down the line which I worry about with my age
The_Doc said:
And whilst this has facts in it, and I don't doubt it as true. It is definitely NOT the picture.
My unit is up to about 1500 of these operations and nobody lost a leg.
.
Precisely my point, I have a narrow skewed view of the procedure as an anaesthetist due to the fact that I have seen one surgeon offering and performing this procedure.My unit is up to about 1500 of these operations and nobody lost a leg.
.
So,
Osteotomy aims to take the pressure away from a worn area of a joint and reduce pain.
Simply put, when the reconstructive and rebuilding options are over (at about age 40, when tissues don't regrow) osteotomy fills the treatment gap..... until joint replacement is a good option.
Joint replacement, either total joint or half a joint (partial knee) is an excellent option, and 90,000 of these are done each year in the UK, they don;t suit the working woman or man.
The replaced joint never really works as well for high intensity labour or sports. And osteotomy does just this.
The weight is taken off the overloaded bearing surface, and as long as the other side/half of the knee is up to the job (and we check) you can put off joint replacement by 10-15 years.
This page, hosted by my good friend, mentor and retiring Chair of the European ESSKA Osteotomy Association, Matt Dawson explains:
https://www.cumbriankneeclinic.co.uk/hto-high-tibi...
What you need to find, if you are not keen or not suitable for joint replacement surgery, is an ecpert in osteotomy.
And they need to be doing 30+ (as a guess) of them a year.
It's a specific skill set. I found that the first 50 or so I did were new territory to me. And this was Matt Dawson in the theatre next to me, he being on 800 procedures by this point !
Ossur Offloader braces are very good and we have them as first line bracing. Offloader One is our choice. They relive pain if offloading is suitable/possible and rehearse the potential benefit of the operation.
We also use offloading braces as a litmus test to see if the offloading would work,
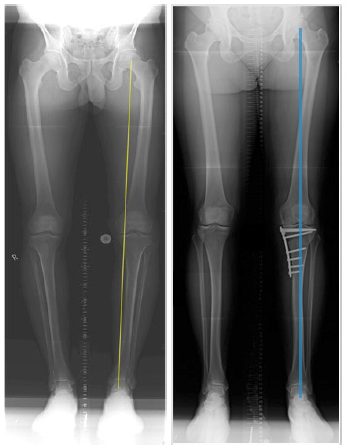
But we also use long leg alignment and CAD planning for the surgery. It's not guesswork.
Bregg offloading also get an honorable mention. Bregg Freestyle is nice.
Of course I'm a convert and fan. I have hundreds of satisfied customers.
But like all surgeons, I see about 5% complication rate, no surgery is perfect. This is is no worse than knee replacement surgery. And the satisfied osteotomy patients are happier.
I don't usually do osteotomy in the over 65s and similarly I never do joint replacement in the under 55s. Each case is different of course. Some surgeons push the envelope. Once you have started on joint replacement though, you can't reverse this decision. Revision replacement is an inevitable next step. Osteotomy puts this back.
Some osteotomies are done for traumatic injuries or serious joint injuries in the younger patient.
Anyhow, back to my hols now.
HTH.
Find an experienced knee surgeon who has osteotomy in his toolbox. A carpenter needs all the tools
ACL is only needed for playing football twice a week or similar pitch pivot sports.
Cadaveric meniscal replacement is for early osteoarthritis and isn't as reliable as osteotomy for pain relief.
Each case is different. I can't help you over the internet.
Osteotomy aims to take the pressure away from a worn area of a joint and reduce pain.
Simply put, when the reconstructive and rebuilding options are over (at about age 40, when tissues don't regrow) osteotomy fills the treatment gap..... until joint replacement is a good option.
Joint replacement, either total joint or half a joint (partial knee) is an excellent option, and 90,000 of these are done each year in the UK, they don;t suit the working woman or man.
The replaced joint never really works as well for high intensity labour or sports. And osteotomy does just this.
The weight is taken off the overloaded bearing surface, and as long as the other side/half of the knee is up to the job (and we check) you can put off joint replacement by 10-15 years.
This page, hosted by my good friend, mentor and retiring Chair of the European ESSKA Osteotomy Association, Matt Dawson explains:
https://www.cumbriankneeclinic.co.uk/hto-high-tibi...
What you need to find, if you are not keen or not suitable for joint replacement surgery, is an ecpert in osteotomy.
And they need to be doing 30+ (as a guess) of them a year.
It's a specific skill set. I found that the first 50 or so I did were new territory to me. And this was Matt Dawson in the theatre next to me, he being on 800 procedures by this point !
Ossur Offloader braces are very good and we have them as first line bracing. Offloader One is our choice. They relive pain if offloading is suitable/possible and rehearse the potential benefit of the operation.
We also use offloading braces as a litmus test to see if the offloading would work,
But we also use long leg alignment and CAD planning for the surgery. It's not guesswork.
Bregg offloading also get an honorable mention. Bregg Freestyle is nice.
Of course I'm a convert and fan. I have hundreds of satisfied customers.
But like all surgeons, I see about 5% complication rate, no surgery is perfect. This is is no worse than knee replacement surgery. And the satisfied osteotomy patients are happier.
I don't usually do osteotomy in the over 65s and similarly I never do joint replacement in the under 55s. Each case is different of course. Some surgeons push the envelope. Once you have started on joint replacement though, you can't reverse this decision. Revision replacement is an inevitable next step. Osteotomy puts this back.
Some osteotomies are done for traumatic injuries or serious joint injuries in the younger patient.
Anyhow, back to my hols now.
HTH.
Find an experienced knee surgeon who has osteotomy in his toolbox. A carpenter needs all the tools
ACL is only needed for playing football twice a week or similar pitch pivot sports.
Cadaveric meniscal replacement is for early osteoarthritis and isn't as reliable as osteotomy for pain relief.
Each case is different. I can't help you over the internet.
Edited by The_Doc on Friday 21st July 16:07
I’m so sorry I completely missed your reply! Thank you so much for such an informative reply…I really appreciate your time taken to reply!
‘Some osteotomies are done for traumatic injuries or serious joint injuries in the younger patients’ I guess this is me, Im significantly under 55 so knee replacement would not be an option.
I’ll look at an offloader brace for them time being and pluck up courage for the surgery
‘Some osteotomies are done for traumatic injuries or serious joint injuries in the younger patients’ I guess this is me, Im significantly under 55 so knee replacement would not be an option.
I’ll look at an offloader brace for them time being and pluck up courage for the surgery
Gassing Station | Health Matters | Top of Page | What's New | My Stuff